Türkçe
Türkçe




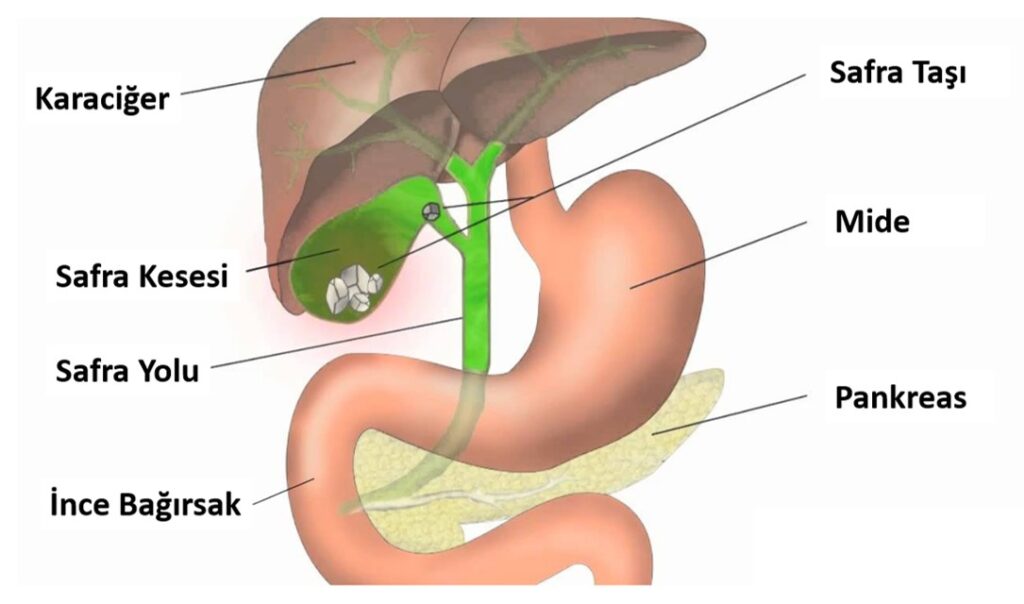
Some of the bile produced in the liver is stored in the gallbladder via the bile ducts and transferred to the duodenum during meals. The prevalence of gallstones in Turkey is 7% in women and 3.5% in men. Approximately 6% of men and 9% of women may have gallstones. The probability of developing complications in patients with asymptomatic gallstones is 2% per year. About 20% of asymptomatic gallstones will become symptomatic after 10 years. These gallstones can progress further and develop complications such as cholecystitis, cholangitis, choledocholithiasis, gallstone pancreatitis and rarely cholangiocarcinoma.
There are three main pathways in gallstone formation: Excess cholesterol produced in the liver forms gallbladder sludge and brown gallstones. Some hematologic diseases cause the liver to produce too much bilirubin and can lead to the formation of black gallstones. If the gallbladder has impaired emptying, bile can condense in it and form gallstones. 90% of gallstones are cholesterol gallstones.
Obesity, age, female gender, pregnancy, genetics, rapid weight loss and certain medications (oral contraceptives, etc.) can cause cholesterol gallstone formation. Patients with cirrhosis, ileal diseases, sickle cell anemia and cystic fibrosis are at risk of developing black pigment stones.
Patients with gallstone disease may have symptoms of biliary colic (intermittent episodes of right upper abdominal pain, often associated with nausea and vomiting), sweating, nausea and vomiting. Fatty meals are a common trigger of gallbladder contraction. The pain usually starts within an hour after a fatty meal and can last for 1-5 hours.
Acute cholecystitis occurs when a gallstone blocks the cystic duct, causing the gallbladder to enlarge and become inflamed. It may be accompanied by fever, pain in the right upper abdomen and tenderness in the gallbladder area (this is called Murphy’s sign). Side effects of cholelithiasis, including acute cholecystitis, cholangitis, pancreatitis, gallbladder empyema, necrosis, gallbladder cancer or other systemic causes, should be investigated.
Blood tests and abdominal ultrasound are performed to evaluate gallstones. Abdominal tomography is useful in the diagnosis of gallstones or cholecystitis to detect inflammation or complications of the pancreas. Tests such as endoscopic or magnetic retrograde cholangiopancreatography can be used when jaundice is present in gallstones.
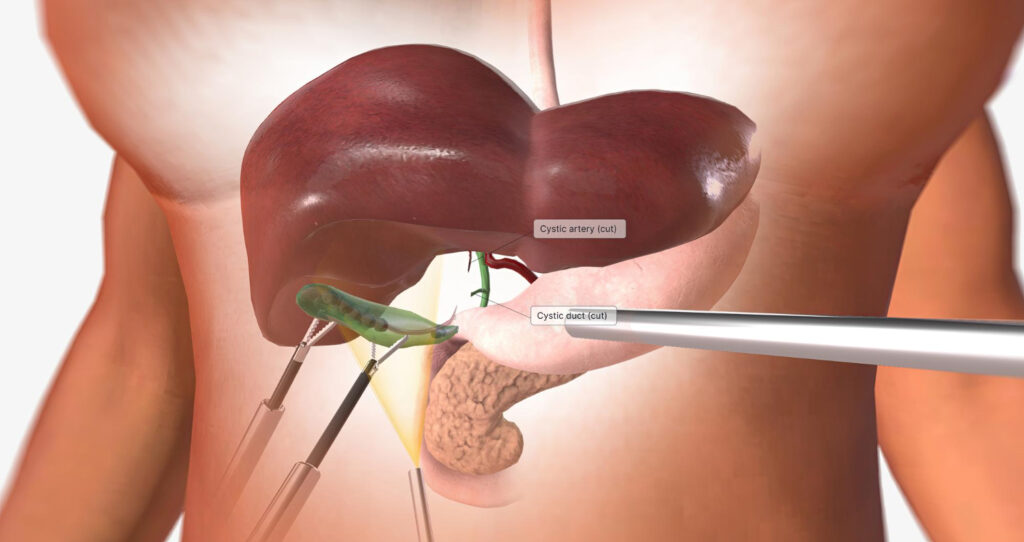
For symptomatic gallstones, once diagnosed, dietary advice should be given to reduce the likelihood of recurrent attacks and referral to a general surgeon for elective laparoscopic cholecystectomy. Today, laparoscopic cholecystectomy is the standard of care and removes the gallstones along with their contents. The operation takes 1 hour and the patient is sent home after 1 day. After 3-4 days, he/she can start his/her daily activities.
Patients with acute cholecystitis will require hospitalization, intravenous antibiotic treatment and emergency surgery if necessary. Medical treatment with Ursodeoxycholic acid as a drug treatment for gallstones is an option but not practical. When the drug is discontinued, there is a high probability of stone formation again.